
Abbey Health PCN
Transforming Long Term Condition Management Through Holistic, Multi-Condition Care
Abbey Health PCN's partnership with Suvera demonstrates how holistic, technology-enabled care can transform long-term condition management.
7.37
mmHg average systolic blood pressure reduction
+10.2%
increase in QOF earnings
88.2%
engagement rate
Summary
Abbey Health PCN's partnership with Suvera demonstrates how holistic, technology-enabled care can transform long-term condition management. By addressing multiple conditions simultaneously through coordinated virtual care, the PCN achieved exceptional clinical outcomes, significant cost savings, and improved operational efficiency. The 88.2% patient engagement rate and substantial improvements across all quality indicators prove that patients respond positively to well-coordinated, accessible care.
This case study exemplifies how innovative healthcare delivery models can successfully manage the growing complexity of multimorbidity whilst providing sustainable, high-quality care that benefits patients, clinicians, and healthcare systems alike.
Pain Points Addressed
Poor Control Rates - Patients not meeting clinical targets
Clinical Capacity - Limited staff time for routine reviews
Patient Engagement - Low attendance or participation rates
Administrative Burden - Manual recalls and coordination
Register Management - Maintaining accurate disease registers
Multimorbidity co-ordination- Managing complex patients with multiple conditions
Cost Pressures - Need to reduce per-patient management costs
Abbey Health PCN serves a relatively affluent population in St Albans across two practices and has faced significant challenges in managing increasingly complex patients with multiple long-term conditions.
The Problem: rising complexity in an ageing population
Abbey Health PCN was grappling with the growing challenge of multimorbidity management and ever-increasing local targets. Their patient population exhibited high rates of multiple long-term conditions, with complex care requirements that traditional approaches struggled to address effectively.
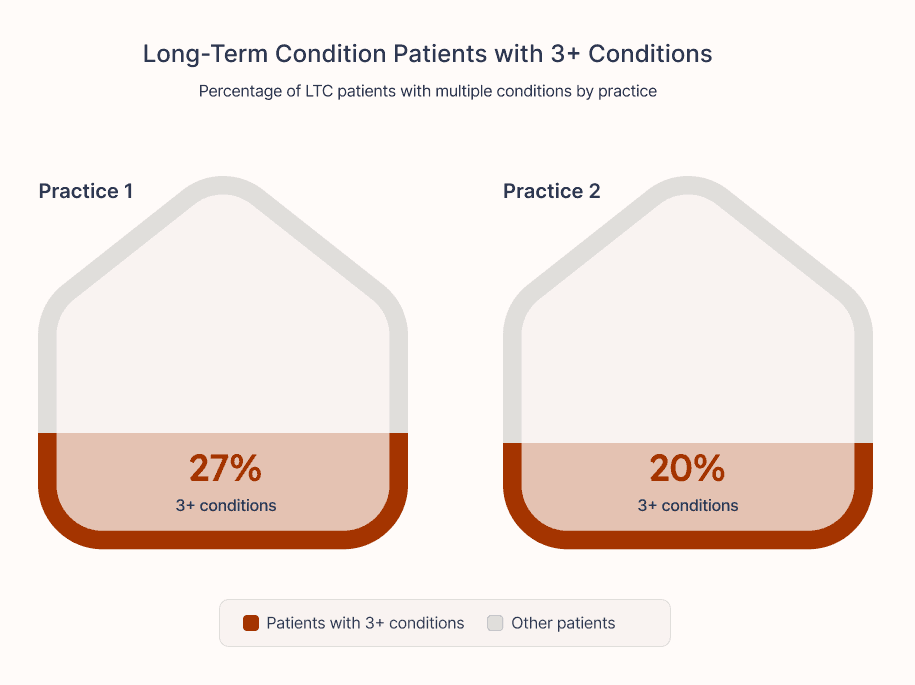
Multimorbidity Statistics:
Practice 1: 27% of LTC patients had 3+ conditions
Practice 2: 20% of LTC patients had 3+ conditions
Patients with single conditions represented only 16% (Practice 1) and 14% (Practice 2) of their LTC population
The PCN was caught in a reactive "end-of-year rush" cycle, chasing Enhanced Care Framework targets without a coordinated strategy. Their uncoordinated approach to long-term condition management resulted in poor control rates, administrative burden, and inefficient use of clinical capacity across both practices. Staff were overwhelmed by manual recalls and fragmented care delivery, whilst patients with multiple conditions often received disjointed care from different services.
Traditional approaches weren't working because they addressed conditions in isolation, creating inefficiencies and gaps in care. The PCN needed a fundamental shift towards holistic, patient-centred management.
The Solution: Suvera's integrated virtual care model
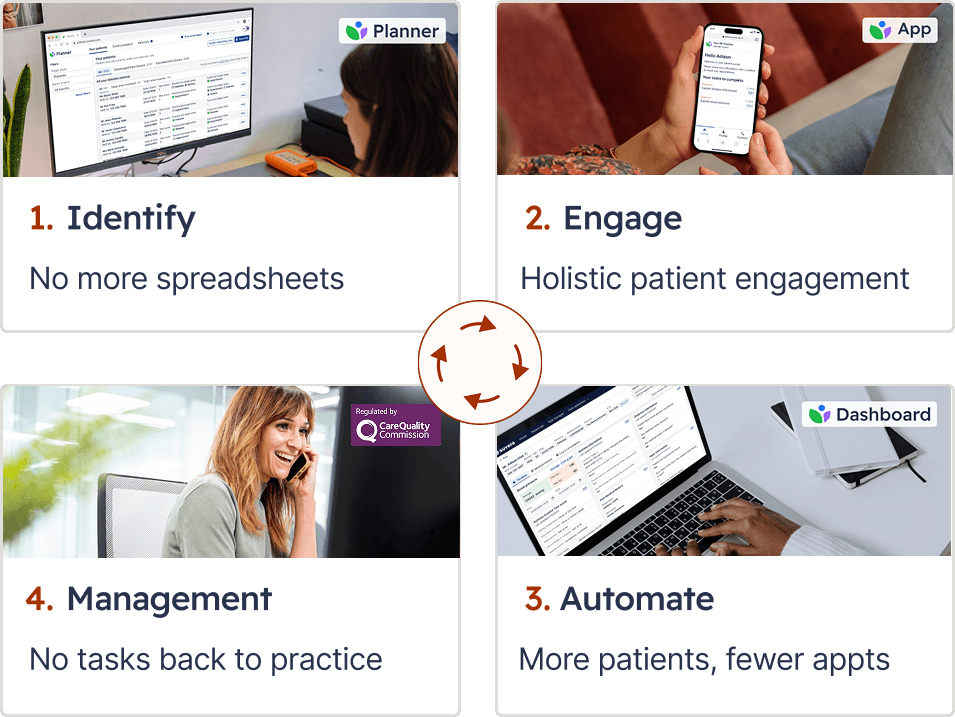
Abbey Health PCN partnered with Suvera to implement a comprehensive, end-to-end strategy for long-term condition management. Suvera's Proactive Virtual Clinics provided:
Core Services:
Virtual consultations (telephone/video)
Home monitoring support with patient WebApp
Automated recall technology through Planner
Urgent case triage within 24 hours
Advanced data analytics and desktop prevalence coding
QOF target management
Local target support (Enhanced Care Framework)
Conditions Managed:
Hypertension
Diabetes
Cholesterol management
Asthma
Non-diabetic hyperglycaemia
Frailty assessments
Structured Medication Reviews
Targeted case finding
Implementation
Suvera implemented a robust segmentation strategy to ensure consistent patient recall and care delivery across both PCN practices:
Month of Birth Recall System: A standardised recall system prevented overwhelming surges in workload whilst promoting efficient resource allocation throughout the year.
Bespoke Workflows: Tailored pathways were developed for each practice, covering routine follow-ups to complex multimorbidity cases, ensuring optimal operation whilst maintaining PCN-wide standards.
Integrated Care Planning: All necessary investigations, including blood tests and foot checks, were coordinated according to each practice's specific requirements, ensuring high-quality, consistent care.
Results
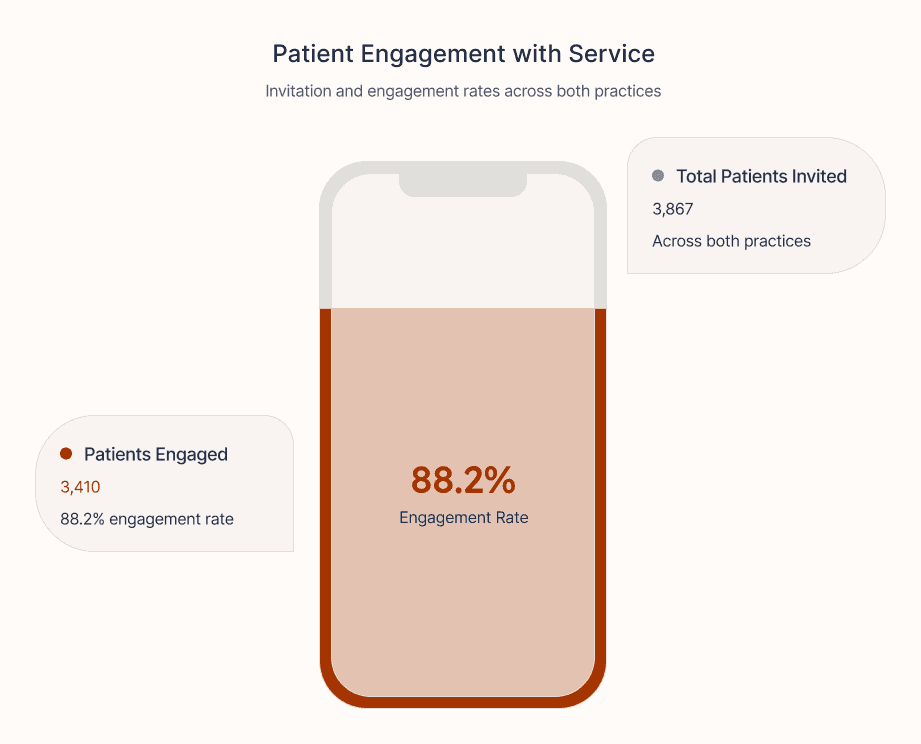
Patient Engagement:
3,867 patients invited across both practices
3,410 patients engaged with the service (88.2% engagement rate)
Blood Pressure Management:
Average systolic blood pressure reduction of 7.37 mmHg
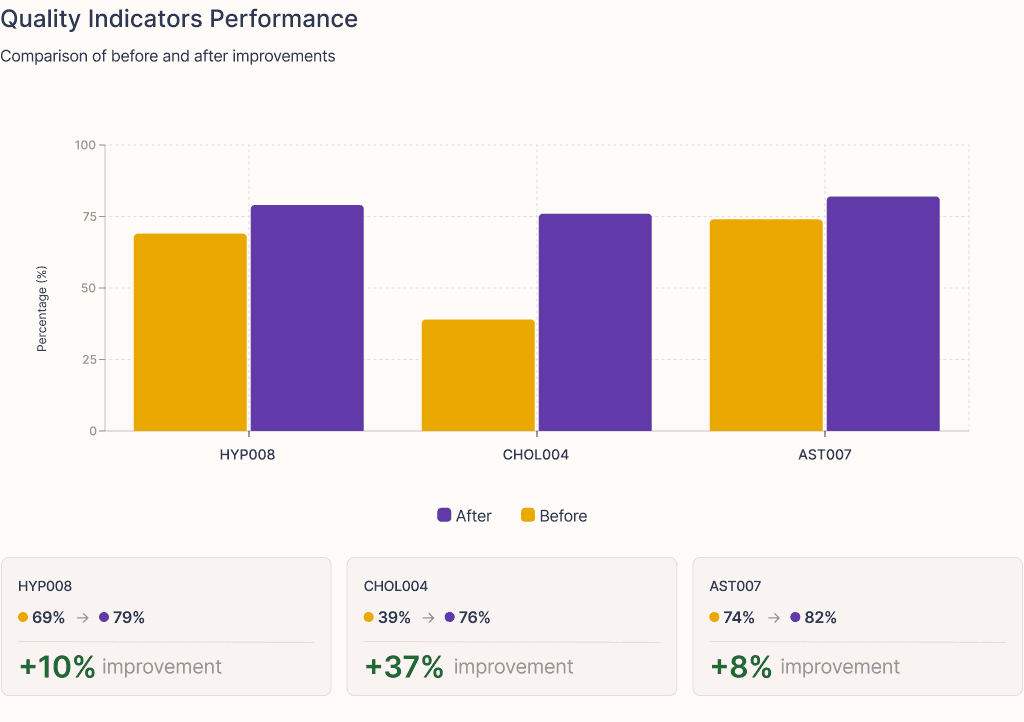
HYP008 quality indicator improved from 69% to 79%
All urgent submissions handled within 24 hours
Diabetes:
Average HbA1c reduction of 11.9 mmol/mol for patients who moved from uncontrolled → controlled following Suvera intervention
Management by Suvera’s care team demonstrates success with drug intervention and lifestyle discussion approaches
Cholesterol:
Average LDL reduction of 1.13 mmol/L
CHOL004 indicator dramatically improved from 39% to 76%
Asthma:
29% of uncontrolled patients were successfully switched to MART therapy
Suvera provided smoking cessation advice to 43% of asthmatics who smoked and who hadn't received GP advice
Significant improvement in Asthma Control Test scores: +3.7 (uncontrolled) and +3.0 (partially controlled)
AST007 improved from 74% to 82%
Hypertension Case-Finding:
300 patients added to the HYP register between 23/24 and 24/25
Systematic identification and addition of previously undiagnosed patients to the hypertension register, improving population health management.
Financial Impact
The transformation delivered substantial financial benefits, with significant savings achieved across the patient journey through Suvera’s identification, recalls, clinical appointments, GP supervision, and software solutions.
Managing 3,867 patients with multiple long term conditions through Suvera's intervention saved significant clinical and administrative time. Without Suvera's support, traditional engagement would have generated ~65% engagement, resulting in 5,028 additional appointments (from 2,514 engaged patients requiring 2 consultations each) and required intensive recall efforts for 1,353 non-engaged patients.
Total hours saved:
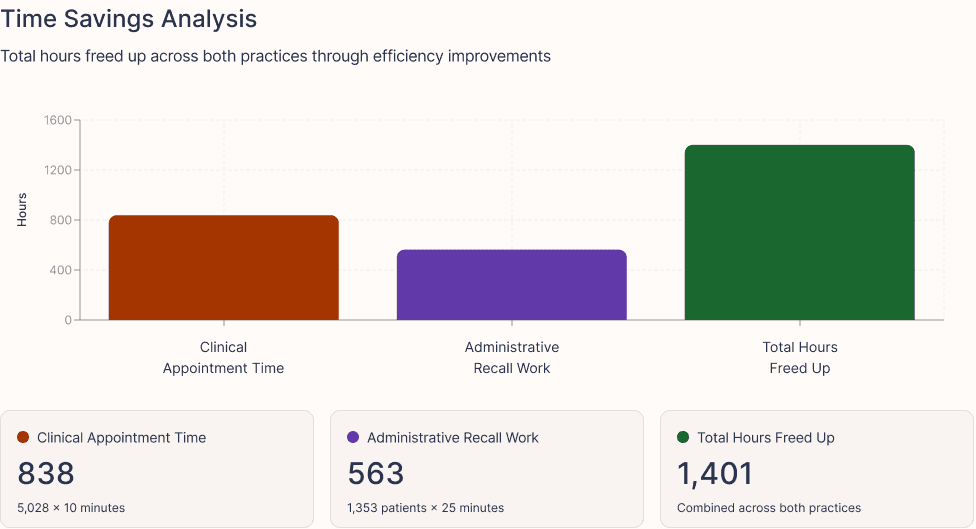
838 hours in clinical appointment time (5,028 × 10 minutes)
563 hours in administrative recall work (1,353 patients × 25 minutes each)
1,401 total hours freed up across both practices
Cost savings:
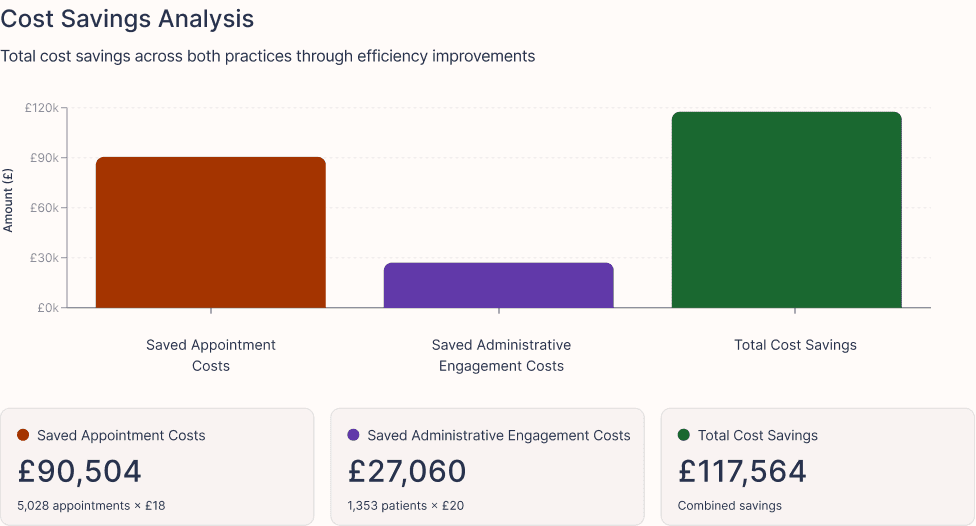
£90,504 in saved appointment costs (5,028 appointments × £18*)
£27,060 in saved administrative engagement costs (1,353 patients × £20**)
£117,564 total cost savings
*£18 is a blended cost of mixed workforce delivering consultations (HCAs, Nurses, Pharmacists, GPs with costs of physical estates, where required).
**With costs for administration, running searches, generating lists, recalling patients and SMS messages, this would cost ~£20 per patient.
Both practices saw an improvement in QOF income for the conditions Suvera was supporting (HYP, CHOL, DM, AST, NDH), with one of the practices seeing a 24% increase in earnings.
Absolute Increase: £9,965
Percentage Improvement: +10.2%
Workforce Benefits
Suvera's Virtual Clinic model and population health Planner technology freed clinical capacity for complex care and other priorities whilst maintaining clinical oversight. Practice teams experienced reduced administrative burden through automated systems, and seamless integration with existing workflows meant minimal disruption during implementation.
To find out how Suvera can support your practice or PCN with long term condition management, get in touch with our team at partnerships@suvera.co.uk
GEOGRAPHY
Urban / Suburban
POPULATION SIZE
30-40k
IMD DECILE
10 (lowest level of deprivation)
ENGLISH SPEAKING %
High
ICB
Hertfordshire and West Essex
KEY DEMOGRAPHICS
High multimorbidity burden


